
Gall bladder and Gall bladder disease management simplified
Gall stones and different problems are commonest the age group between 35- 55 years. However, one can have this as a newborn or even in old age; 80’s and 90’s.
Author has 30 years’ experience of Laparoscopic surgery and he is a teacher and trainer in United Kingdom, Europe, Middle East and Asia in Gall Bladder disease surgery
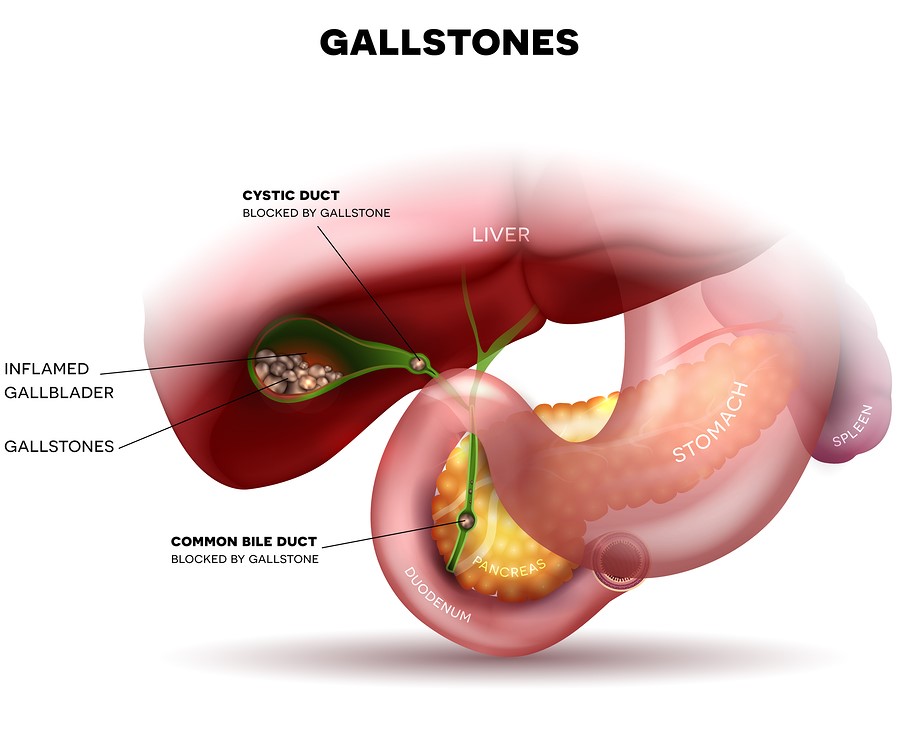
Gallstones, medically known as cholelithiasis, are small or large stones present in the gall bladder. Gall stones can be very small or large, single or multiple. Mostly the gallstones have a smooth surface. The colour can range from pale whitish (cholesterol stones) to dark brown (Bile stones)
Bile which causes gallstones, is a golden/yellow colour liquid produced in the liver; about 1/2 to 1 liter in a day. It leaves the liver through the tubes (right and left hepatic ducts), most of it enters the small intestine directly, some enters the gall bladder where it is concentrated. Whenever signals get to gall bladder after eating food, gall bladder contracts and the bile from the gall bladder flows into the duodenum (small bowel).
Bile helps to break the fat in food into smaller particles like “dish washing liquids cutting the grease, making it easier for water to wash it away.” The digestion of fat in the gut is carried out by enzymes from the gland pancreas.
Gall bladder is a small pear size organ attached to the lower surface of liver under the ribs on the right side. Its capacity is only 50-70 mls. It is attached to the main tube (common bile duct) connecting the liver to the duodenum (small bowel). Its function is to store some bile.
There can me many reasons for formation of gallstones in the gall bladder. Infection of gall bladder, infection of bile, poor contraction or obstruction of gall bladder and changes in the constituents of the bile are some of the common causes.
Pain from gallstones is triggered by eating a fatty meal. Fatty meal causes strong contraction of gall bladder on the stones. It’s like walking on a pebble beach without slippers. At times a stone may become impacted in the outlet (neck) of gall bladder and pain continues for longer time.
Symptoms of Gallstones can vary from vague indigestion symptoms to severe pain, fever necessitating hospital admission. Pain from gallstones generally occurs in the right upper abdomen and it radiates to the back between the shoulder blades. Sometimes the pain from gallstones can just be in upper abdomen without radiating to the back.
The pain is severe and females often describe this as worse than labour pain.
Not all gallstones cause symptoms and many remain asymptomatic and one may not be aware of their presence. These come to light when an ultrasound (scan similar to done for pregnancy) is done for some other reason s that biliary pain.

- Symptoms and complications of Gallstones when inside the gallbladder:
These can cause vague symptoms as nausea, change in taste or mild fever.
Flatulent Dyspepsia
Commonly observed in obese, fatty women complaining of heartburn, abdominal discomfort, belching and fatty food intolerance.
Pain / Gallstone colic
Medically termed as biliary colic. Its Severe, colicky pain felt mostly in the upper abdomen. Pain can shoot to the back or between the shoulder blades often associated with vomiting, restlessness, and sweating. Strong pain killers, clinical assessment and sometimes admission in the hospital is required.
Dyskinesia of gallbladder (poorly contracting gallbladder):
Patients can have gall bladder pain even without gallstones. Specialist surgical opinion will help to solve this mystery; which can be debilitating for patients and can take a long time to diagnose.
Infection / Inflammation
Acute Cholecystitis in medical terms occurs when a gallstone gets lodged in the neck of the gallbladder (Hartmann’s pouch), causing bile stasis leading to gallbladder inflammation. Cholecystitis is an acute condition and can cause severe pain, vomiting, nausea, and fever. Strong pain killers, clinical assessment, blood tests, antibiotics and admission in the hospital is required.
Acalculous Cholecystitis (Infection of Gall bladder without any stones):
This condition is noted in very sick patients and requires specialist input of an experienced surgeon. What may look like an inflamed gallbladder on scan be a gangrenous gall bladder.
Blocked Gall Bladder/ Mucocele
It occurs when a stone is completely blocking the gall bladder outlet blocking the cystic duct or the Hartman’s pouch, but there is no infection. This leads to a distension of the gall bladder and pain. One notices “white bile” in the gall bladder at surgery. Surgery is required in this situation.
Abscess/ Empyema
It’s a completely blocked gall bladder like a mucocele with superadded infection as well. Its like an abscess, where simple antibiotics will not work. Emergency decompression or removal of gall bladder is required after appropriate assessment by a surgeon in a hospital.
Perforation of gall bladder
Perforation (rupture) in abdominal cavity is a rare condition. Impacted stone, diabetes, or virus can precipitate an empyema causing gangrene of gallbladder and perforation.
High-grade fever, chills, and pain in the abdomen are common symptoms. Emergency treatment in a hospital with immediate surgery can be lifesaving in this situation.
Fistula formation (Leak into another organ):
In case on chronic cholecystitis a stone in gall bladder can erode into duodenum or large bowel, leading to Cholecystoduodenal fistula or a Cholecystocolonic fistula. This can happen silently and may come to attention while having tests done for any reason. Generally these can be left alone and observed it not giving any symptoms to the patient.
Mirizzi’s Syndrome:
A stone impacted in the Hartman’s pouch or the cystic duct if not causing a full blockage of the gallbladder outlet can keep getting bigger and can fistulate (erode) into the common bile duct. This can lead to pain, infection, jaundice or even sepsis and requires input from a specialist surgeon urgently. This should ideally be dealt with Laparoscopically and may also require an ERCP (Endoscopic Retrograde Cholangio Pancreaticography).
Small bowel Obstruction / Gallstone Ileus:
A large gallstone escaping the gall bladder due to Cholecystoduodenal fistula can get impacted in small bowel and cause a complete blockage requiring emergency surgery to relive the obstruction and remove the gallstone from small bowel.
Gallbladder Cancer:
The likelihood of cancer is not common, but chronic cholecystitis or cholelithiasis can pose an increased risk of gallbladder cancer. Gallbladder polyps and Porcelain gall bladder are also considered as risk factors for gallbladder cancer.
Gall Bladder cancer carries a poor prognosis.
- Complications of Gallstones in the Common Bile Duct (CBD)
Though the complications are fewer than of the stones within the gallbladder but these are much more serious and potentially life threatening.
Obstructive Jaundice:
Obstruction to the bile outflow causes obstructive jaundice. Jaundice with yellow skin, yellow eyes, dark colored urine, clay-colored stools, and itching are the usual symptoms.
One need to see a surgeon to get the advice and treatment.
Generally, one requires ERCP and Laparoscopic Cholecystectomy.
Cholangitis:
It is the bacterial infection of common bile duct causing abdominal tenderness, chills, fever, and rigors. This is a very scary situation for the patient and requires urgent attention, admission in the hospital and antibiotic treatment with appropriate decompression of the system.
Gallstones Pancreatitis
There is no greater or worse complication of gallstones than acute pancreatitis or inflammation of pancreas due to a gallstone blocking the common opening of the common bile duct with the pancreatic duct.
Patient requires emergency admission in the hospital and appropriate care, investigations and treatment.
In mild pancreatitis one may get better in a day or two. In moderate cases one may lose the function of pancreas and become diabetic for life long. In some cases of severe pancreatitis, this may me life threatening.
Clinicians suggesting or patients considering wait and watch on their gallstones must consider this small but potentially life-threatening complications of gallstones in their mind.
SEEKING MEDICAL ADVICE
Gallstone pain can wax and wane. It can remain asymptomatic for long periods of time but can always flare up unexpectedly. Seeking medical opinion on time is beneficial in terms of health, time, resources and avoiding complications.
If you are experiencing any of these symptoms, then see a doctor immediately.
- Nausea and vomiting
- Prolonged abdominal pain lasting more than 4 hours
- Fever
- Chills and rigors
- Yellowish tinge in the white of the eyes or skin
- Clay-colored stools
- Fatty food intolerance
- Dark-colored urine
Temporary measures:
Exercise and high-fiber, low-fat diet prevents gallstones may reduce the pain flare ups in gallstone patients. For gallstone patients, this is a temporary treatment option while waiting for a definitive medical intervention, which is necessary to avoid any complication.
- Medical Treatment
Medical Treatment was suitable only for some small stones. Once popular in 1970’s it is not used anymore. Medication was used to dissolve stones. Medicine had to be used for many months or a few years. Soon after stopping the medication patients would get stone recurrence.
- Shock Wave Lithotripsy (SWL)
While useful in Kidney stone SWL or Laser treatments are not an option for stones in
the gallbladder.
- Olive oil remedies, mixtures as mentioned on social media
These are not recommended and can be very dangerous if strong contraction of the gallbladder will expel the stone on the common bile duct, thus causing with potential complications alike acute pancreatitis, which could be life threatening.
- Surgical Treatment
- Surgical removal is the standard treatment option for gallstones. This can be offered safely in experienced hands and prevents complications and the complete removal of gallstones. Chose a good surgeon working in a decent hospital.
- Operation in the form of Laparoscopic Cholecystectomy (key hole operation) is the most commonly performed surgical procedure that involves four small cuts in the abdomen. A laparoscope (a camera with light source) is introduced in the abdomen. The surgeon Introduces 3 fine instruments, not much thicker than chopsticks to separate the gallbladder from the adjoining organs and remove it carefully through one of the small incisions.
Laparoscopic Cholecystectomy is a minimally invasive procedure which is done as one-night stay in the hospital. This can be performed in suitable patients as day case as well.
RISKS OF WAITING
- Acute gallbladder inflammation (cholecystitis)
- Bile duct stone (choledocholithiasis)
- Acute bacterial infection (cholangitis)
- Pancreatic infection (pancreatitis)
- Perforation of gall bladder
- Cholangitis (severe infection)
SURGICAL RISKS FACTORS
Laparoscopic Cholecystectomy is well established for more than 30 years. It is performed under full general anaesthetic. It takes a good surgeon and team about 15 – 25 minutes to perform a standard Laparoscopic Cholecystectomy.
Prior to this the operation of removal of gall bladder was done with long open cut just below the right ribcage. Hospital stay used to be 5-7 days after surgery and recovery would take weeks.
Risks of Cholecystectomy open or Laparoscopic are:
- Bleeding
- Damage to the neighboring organs such as liver or intestine
- Damage to common bile duct (very serious complication)
- Postoperative infection
- Postoperative pain
No surgery should be taken lightly. The above-mentioned risks all combined are quoted as less than 1%. The complications mentioned can be severe, may require a reoperation. The complication of damage to common bile duct is very serious indeed and much more common than generally quoted. Even in United Kingdom its incidence is 1:250, which unfortunately is unacceptably too high.
In experienced hands of specialist upper Gastro Intestinal (Upper GI) surgeons the incidence of damage to common bile duct will lower than 1:1000. Ask your surgeon his personal incidence of damage to common bile duct.
In case of this rare occurrence in upper GI surgeon’s hands they ae able to reocgnise it and deal with this skillfully and in a timely fashion.
GOLD STANDARD TREATMENT FOR GALLSTONES
In general, laparoscopic cholecystectomy has been the gold standard for gallstone treatment. It has fewer complications, rapid recovery, less post-op pain, early mobilisation, return to driving, and early return to work and exercise.
New Gold Standard for Cholecystectomy
Currently MiniScarLess (MSL) Cholecystectomy an innovation by the author Professor Amir Nisar, being offered in Mediclinic Parkview hospital, has some further benefits over and above the conventional Laparoscopic Cholecystectomy in terms of cosmesis, less post-operative pain, early recovery and return to exercise and work. Patient experience has been excellent after MiniScarLess (MSL) Cholecystectomy.