“Innovations are the blazing trail of the Eureka moments illuminating our life, work and living. Eureka moments are not man made, rather God’s gift to mankind through his chosen ones. Innovators must maintain humility and remember that glory is only for the creator: Allah, the most magnificent”
"Skin is our outermost garment and deserves the utmost care, love and very well considered gentle handling like inside of the body"
Professor Amir Nisar takes great pride in achieving excellent cosmetic outcomes for his patients after surgery. Hence, it tops his list of innovations.
A fine skin closure with his innovative approaches (3 in number) mostly gives a nice surprise to the patients after surgery.
Mini Scar Less (MSL) surgery and innovative Amir’s dermoplastic approach provides excellent outcomes in majority of the cases.
(Innovations # 2-3: for Reflux / Heartburn after Bariatric (weight Loss) Surgery)
2
Anti-Reflux Surgery after Obesity Surgery / Sleeve Gastrectomy
“ADR- The Gold Standard to treat reflux after Weight Loss Surgery ”
Amir’s Dubai Repair -ADR.
Heartburn or Reflux after weight loss surgery like sleeve gastrectomy is a complex issue and difficult to mange.Amir’s Dubai Repair -ADR is an effective and simple solution to this debilitating problem.
Anti-Reflux Surgery after Obesity Surgery / Gastric Bypass Surgery
“ADR- The Gold Standard to treat reflux after Weight Loss Surgery ”
Amir’s Dubai Repair – (ADR) For Heartburn After Sleeve Gastrectomy/Gastric Bypass
Heartburn or Reflux after weight loss surgery like Gastric Bypass is a complex issue and difficult to mange.Amir’s Dubai Repair -ADR is an effective and simple solution to this debilitating problem.
Mini-Scar-Less (MSL) Laparoscopic Nissen’s Fundoplication; Amir modified technique with Amir’s surgical Protocol.
“ There is no other operation more beautiful, satisfying, life changing and yet so challenging like anti reflux surgery ”
Professor Amir Nisar is very proud of this innovation helping hundreds of patients in his practice. This is the least invasive antireflux technique o deal with heartburn. The accumulative length of the incisions is 1.6 cms. The standard and quality of the surgery remains the same as with conventional Laparoscopic surgery. Recovery is wuick and cosmesis is excellent.
Needlescopic 3 port Nissen’s Fundoplication; Amir modified technique with Amir’s surgical Protocol
“ There is no other operation more beautiful, satisfying, life changing and yet so challenging like anti reflux surgery ”
“Unique challenges require innovative responses”
A very special bespoke technique developed in 2008 by Professor Amir Nisar for a European kick boxing champion, who suffered from severe reflux. With least number of Strategically placed smallest possible cuts on abdomen, the recovery is quick and return to professional fights with tolerance of punches and kicks being thrown on tummy is excellent.
Professor Amir Nisar developed this technique in Kent, United Kingdom and later shared this on meetings and conferences in United Kingdom, Europe and Asia.
First 20 Day Case Laparoscopic Nissen’s Fundoplications in the world
“Professor Amir Nisar’s one of many first”
First time ever, “Day Case” Laparoscopic Nissen’s Fundoplications along with Professor Michael Bailey, Guildford, Surrey, United Kingdom. With mean post operative stay of 5.4 hours in the hospital before being discharged home proved to be a bench mark for day case Laparoscopic Surgery in United Kingdom and all over the world.
With more efficient and effective approaches hernias and gall bladder surgery was being done prior to our successful day case Laparoscopic Nissen’s Fundoplication surgery. However, performing complex surgery like Laparoscopic Nissen’s Fundoplication further improved the standards of Laparoscopic Hernia surgery and Laparoscopic Gall Bladder Surgery. Our center’s results were 96% Hernias and 85% Gall Bladder surgeries as day cases. In order to achieve this we worked hard at the teams, techniques and pathways: patient safety is paramount.
“Always at the forefront of surgery”
Professor Amir Nisar was one of the chosen/designated few surgeons from United Kingdom operating on the National Reflux Multicenter Trial in UK in 1999/2000.
He performed simple and complex Giant Hiatal Hernias for the trail with his innovative methods and contributed towards the excellent results of the trial, proving that Laparoscopic Nissen’s Fundoplication is effective surgical option for heartburn/ Reflux.
Laparoscopic Nissen’s Fundoplication has been hailed as Gold standard for reflux treatment since.
Gastroscopy / Endoscopic assessment of Complications after Anti-Reflux and weight loss Surgery
“Diagnostic endoscopy is the mainstay of assessment for complications after ant-reflux or weight loss surgery, a surgeon with surgical knowhow and excellent endoscopic skills can get the answers and plan strategy to deal with the issues in the best possible way”
Professor Amir Nisar recognised the short comings of standard endoscopy in assessing the complications of previous anti-reflux or weight loss surgery. He developed the technique of “Gasless endoscopy” in 2001. He managed to assess the slipped wraps and its correlation to hiatus effectively with this approach. He has presented his technique of gasless endoscopy widely in UK and Europe on International forum for accurate assessment for complications like dysphagia or recurrent reflux after anti reflux surgery.
There are about 14 different surgical or endoscopic options to treat reflux in patients with heartburn. Laparoscopic Nissen’s Fundoplication offers the best outcomes in terms of control of reflux in short, medium and long term. All other operations are far behind.
This special and innovative technique of Professor Amir Nisar addresses the issue of reflux returning after a few decades of original Laparoscopic Nissen’s Fundoplication.
“Touching the inside of patient with cotton wool should be every surgeon’s aim”
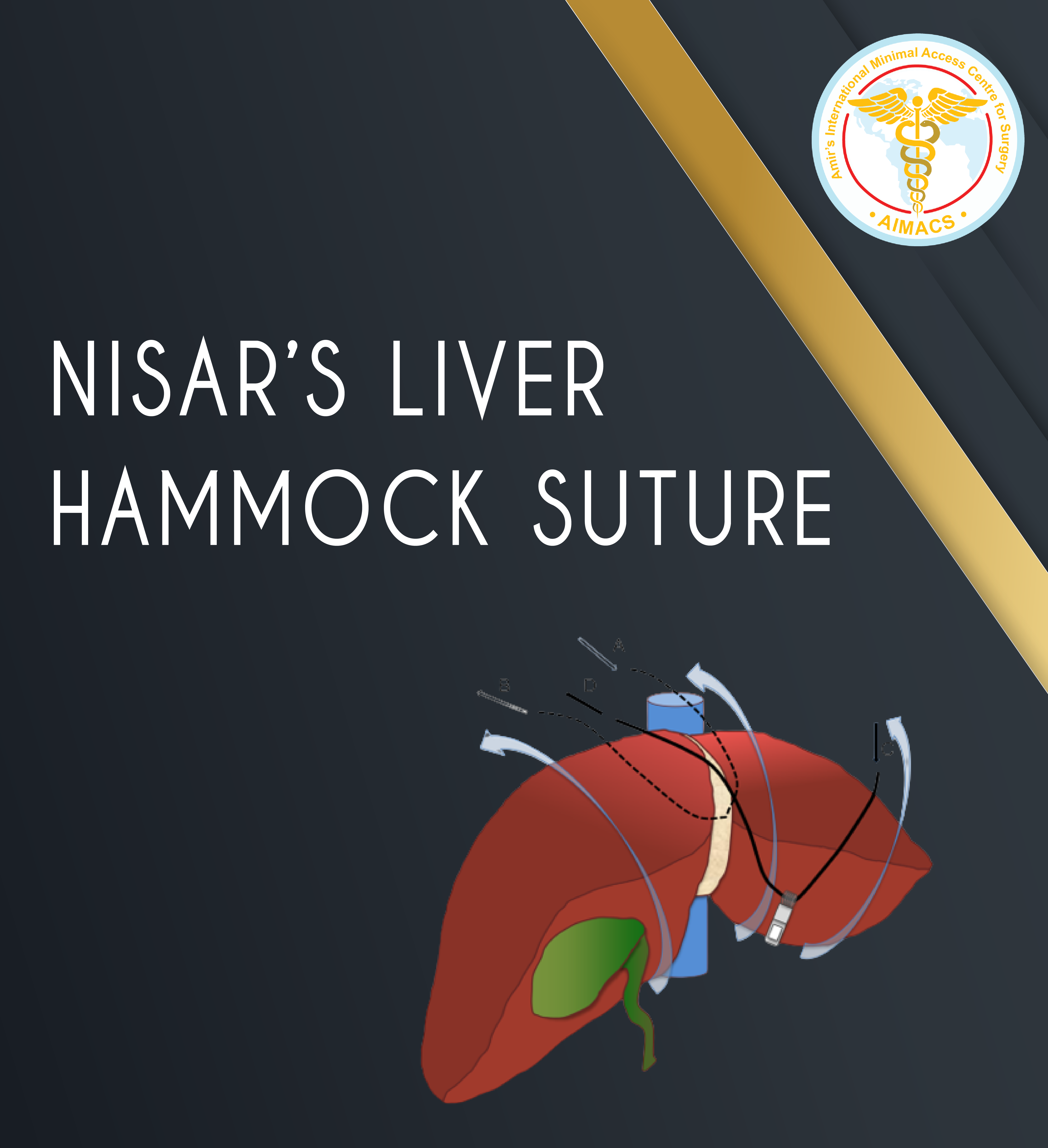
For Laparoscopic Nissen’s Fundoplication a steel retractor is used to left up the left lobe of the liver to gain access and visibility of Hiatus and hiatus hernia. This retractor being in position (45 minutes to 3 hours) for the duration of surgery causes significant liver congestion. The pressure on liver and congestion causes significant post operative pain and deranged liver functions post operatively which may take up to a week to improve, thus adding on to the trauma of real surgery and delayed recovery with higher pain scores.
“Nisar’s Liver Hammock Suture is Professor Amir Nisar’s Innovation for more than 14 years and he uses this in most of his cases with great benefit for the patients. Liver sits over this innovative retraction hammock and is as healthy and fresh looking as at the start of the operation. Patients experience no pain for the liver retraction and their Liver enzymes also remain normal. No doubt that the recover is quick with much less pain than traditional liver retraction. Professor Amir Nisar has shared his innovation on many courses and meeting globally for the benefit of patients worldwide.
“Poor understanding of Hiatal repair of a hiatus hernia and subsequent repair is “Achilles heel of Anti-reflux surgery”
Professor Amir Nisar
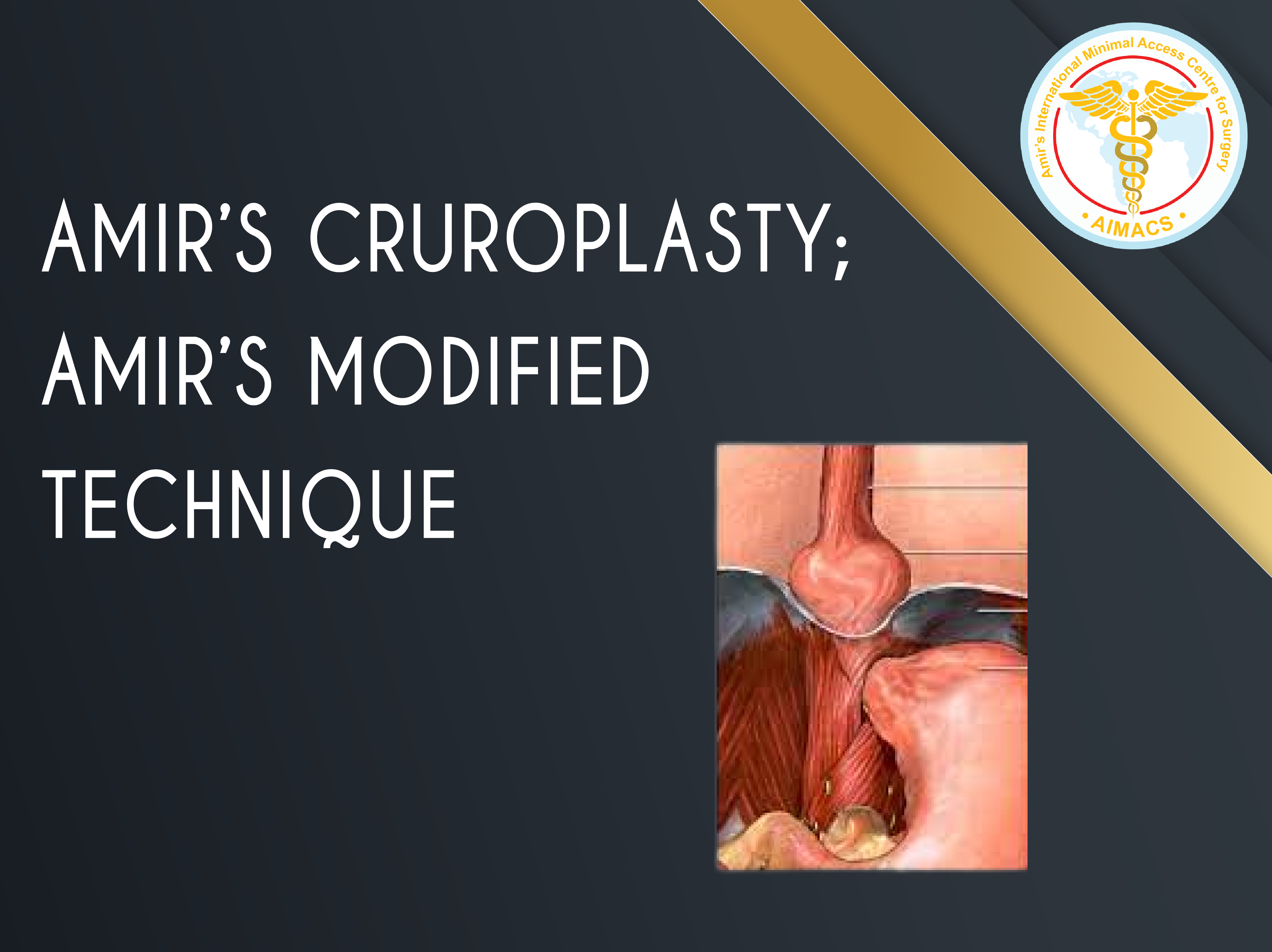
Professor Amir Nisar’s great interest in human anatomy has made him a life long student of human body – “Allah has created human body with great precision – Surah e Teen”. We as humans have only touched the surface and understood it superficially so far. Knowing the anatomy and variations of crurae and taking the fine variations into considerations helps a master surgeon to get an ideal and long lasting control (repair) of this very dynamic area (Hiatus), which can get various distractions and movements for up to 30, 000 times every day!
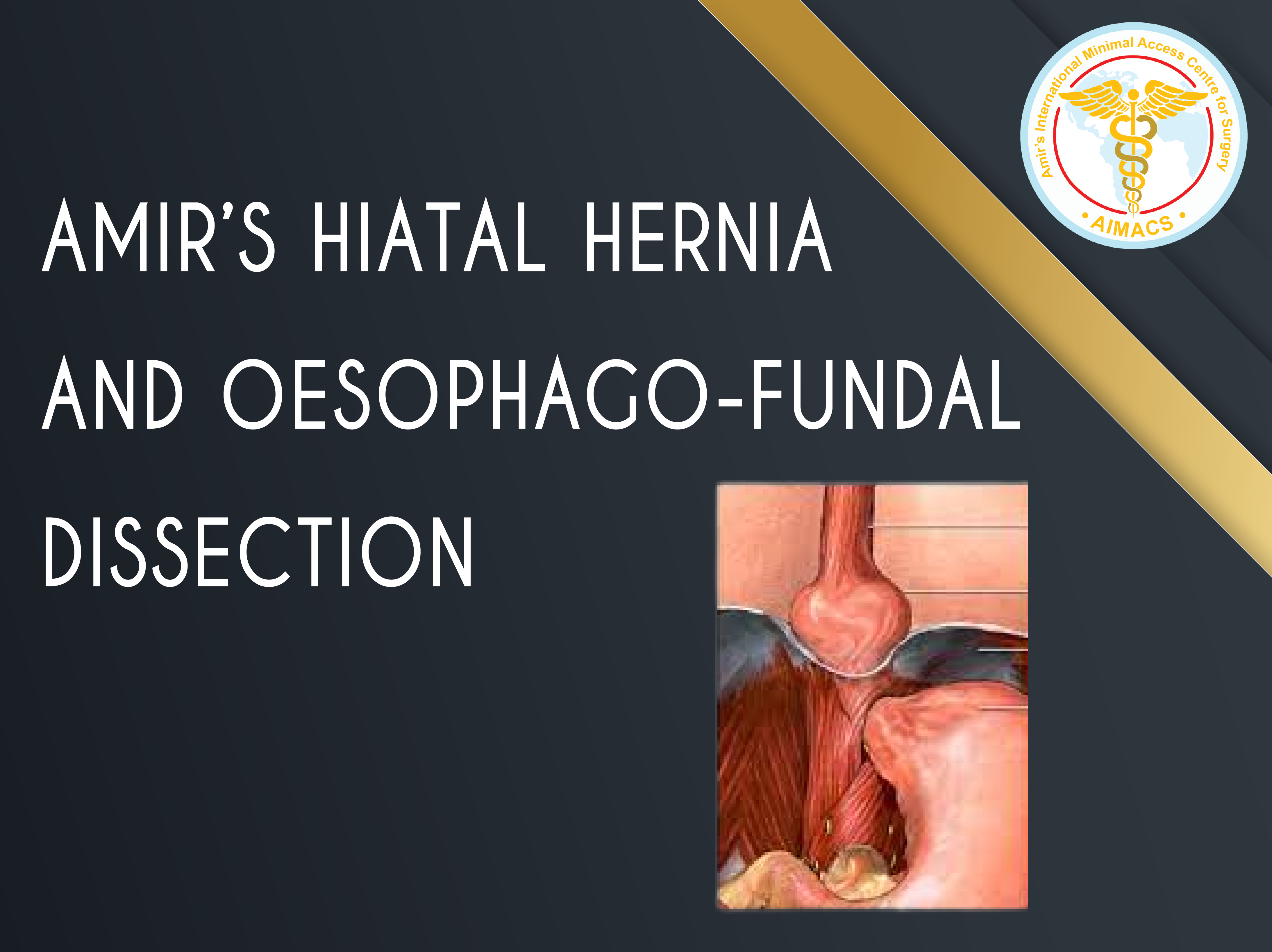
Amir’s Hiatal hernia and Oesophago-fundal dissection
“The balance of a perfect mobilisation is very delicate while performing a fundoplication (for anti-reflux surgery). A few centimeters less or more can tip the balance; a failure of surgical outcome”
There are crucial areas that need to be mobilised and similarly other key areas that should be left untouched: four to be precise (Oesophageal, Hiatal, Fundal and OesophagoFundal). Lack of judgment lead to increased risk of post operative complications and failure of surgery.
Professor Amir Nisar has defined and identified these precisely and thousands of his patients has benefitted for more than two decades due to this precision.
“Grand Finale of Laparoscopic Nissen’s Fundoplication”
While each of 37 steps in a Laparoscopic Nissen’s Fundoplication is crucial: none more than the final wrap setting and positioning. This is crucial in terms of avoiding some complications of dysphagia due to “Bean and doughnut effect”; terms coined by Professor Nisar after his observation in these subtle issues during surgery in 2006. Patients with bean and doughnut effect suffer from dysphagia which is extremely difficult to detect by routine investigations. A stitch in time saves nine.
“A door’s hinges fixation, longevity and function should be as long as the building itself”
Professor Amir Nisar
With experience of nearly 3 decades in Ant-Reflux surgery and Laparoscopic Nissen’s fundoplication and assessments of pitfalls after the complications of previous surgery, referred to him in tertiary referral centers, Professor Amir Nisar has innovated a standardised “Diamond and cape” technique to prevent wrap slippage, wrap migration, post operative dysphagia, recurrent reflux and Pseudo dysphagia in patients undergoing Laparoscopic Nissen’s Fundoplication; hence the term “Laparoscopic Nissen’s Fundoplication; “380 degrees” – Amir modified technique”.
This innovative technique is particularly helpful in achieving excellent long term results in patients who are old, malnourished, on steroid or immune suppressive therapy, suffer from chronic cough, asthma or become pregnant after initial surgery.
Laparoscopic Anti Reflux operating for Giant Hiatal Hernias
“Giant Hiatal hernias ("full stomach in the chest”) are of 3 types: Reducible, Sliders and fixed”
Professor Amir Nisar has worked in high volume tertiary referral centers in United Kingdom for 25 years and has dealt with many complex operations. Giant hiatal hernias present unique challenge. Professor Amir realised that conventional approach did not meet the demands of this complex situation. He has developed a unique approach to effectively deal with Gian Hiatal hernias and gastric volvulus, thus making the operation straight forward, requiring less operative time and providing excellent repair.
Eagle Claw” retraction of Omentum in Obese patients for Oesophagogastric and Colonic surgery.
"Eagle Claw is like having 5 hands inside the abdomen for retraction"
Precise and effective retraction of tissue in laparoscopic surgery for appropriate visibility and access to organs is paramount. This innovation helps in difficult scenarios and halps to perform surgery with an appropriate and clear vision.
“While the pain has come down from 6/10 from open surgery to 3/10 of Laparoscopic surgery: it should be 0-1/10”
Since 2001, Professor Amir Nisar has continually pondered over the issue of pain after Laparoscopic surgery. He has many innovative techniques and procedures to minimise pain after Laparoscopic Anti Reflux Surgery. This enhances his patient’s experience and is very satisfying for himself and his co-workers caring for the patients.
18
No starvation: Early Feeding after Laparoscopic Nissen’s Fundoplication -
“I put your money where my mouth is”
Professor Amir Nisar does not keep his patients on liquid or modified diet for too long like most other surgeons performing anti-reflux surgery.
Patients are fed soft food on the day of surgery building up to nearly normal diet withing two weeks of surgery. This avoids prolonged starvation, resultant fatigue and slow recovery
Though not precisely an innovation in itself; but the cumulative byproduct of all the innovations listed above.
Minimal Invasive Inguinal/ Umbilical and Incisional Hernia Surgery
“Hernia Surgery is a master surgeon’s craft: a specialty in itself” – Professor Amir Nisar
19
Laparoscopic Totally Extra Peritoneal (TEP) Inguinal Hernia repair for Incarcerated Sliding inguinoscrotal hernia
The first case in the world performed in 1999; case series presented in ALSGBI annual meeting, Hull, United Kingdom in 2002 and EAES annual meeting in 2003.
“Millions of hernias are being done globally every year by thousands of surgeons: an innovation and breakthrough in this area of surgery is truly Allah’s gift to mankind”
Incarcerated Sliding inguinoscrotal hernias are always challenging and were considered inoperable with TEP approach prior to this innovative technique. Professor Amir Nisar not only demonstrated his innovative technique to deal with the challenge but also highlighted some mis-concepts among the surgical fraternity regarding incarcerated Sliding inguinoscrotal hernias. His presentation is 2003 Venice, Italy titled Anatomical basis of Sliding inguinal hernias” was well received and is helpful for surgeons performing even open sliding hernias. His take home message was threefold:
Sliding Inguinal hernia operations are not complex; only anatomy is poorly understood.
A sac can always be opened in a sliding inguinal hernia with an open or TEP approach and there is no risk to damage to the slider sigmoid colon or caecum in the Inguinal canal.
Sac amputation after its opening and reduction of hernia is far better in open and laparoscopic approaches rather than complete dissection of the sac and its reduction, as practiced tradionally.
Sac amputation in Laparoscopic Totally Extra Peritoneal (TEP) Inguinal Hernia repair
Long Inguinoscrotal inguinal hernias are challenging during laparoscopic repair. Three fine tricks devised by Professor Amir Nisar makes them easy to handle.
Mini-Scar-Less (MSL) Inguinal hernia Totally Extra Peritoneal Repair (TEP) repair
This is the least invasive approach for inguinal hernia surgery anywhere in the world. Accumulative length of incisions is approximately 1cm for bilateral Inguinal hernia operation!
Its an excellent technique for quick recovery and least pain after surgery.
Patients do not need to avoid exercise after surgery. Return to driving, lifting weight and exercise in minimal.
“While the pain has come down from 6/10 from open surgery to 3/10 of Laparoscopic surgery: it should be 0-1/10”
Since 2001, Professor Amir Nisar has continually pondered over the issue of pain after Laparoscopic surgery. He has many innovative techniques and procedures to minimise pain after Laparoscopic Inguinal hernia surgery. This enhances his patient’s experience and is very satisfying for himself and his co-workers caring for the patients.
(Innovations # 26-27: Gall bladder / Gallstones disease Surgery)
Laparoscopic Gall Bladder Surgery/ Laparoscopic Cholecystectomy
“Gall Bladder Surgery though common should only be performed by specialist upper Gastro Intestinal and hepatobiliary surgeons” ; Professor Amir Nisar
26
Mini-Scar-less (MSL) Laparoscopic Cholecystectomy for Gall Bladder Disease. Clipless and Scarless operation; good for better cosmesis and less post operative pain and quick recovery.
“While the pain has come down from 6/10 from open surgery to 3/10 of Laparoscopic surgery: it should be 0-1/10”
Since 2001, Professor Amir Nisar has continually pondered over the issue of pain after Laparoscopic surgery. He has many innovative techniques and procedures to minimise pain after Laparoscopic Gall Bladder Surgery. This enhances his patient’s experience and is very satisfying for himself and his co-workers caring for the patients.
“Though a common operation: deserves due attention and better approaches than commonly practiced” – Professor Amir Nisar
28
Mini-Scar-less (MSL) Appendicectomy
Surgery with least noticeable scars; particularly appealing for young children and females. Less pain and early recovery preferable to all genders and all ages.
Needlescopic Appendicectomy is also better approach than conventional Laparoscopic surgery
“While the pain has come down from 6/10 from open surgery to 3/10 of Laparoscopic surgery: it should be 0-1/10”
Since 2001, Professor Amir Nisar has continually pondered over the issue of pain after Laparoscopic surgery. He has many innovative techniques and procedures to minimise pain after Laparoscopic Appendicectomy Surgery. This enhances his patient’s experience and is very satisfying for himself and his co-workers caring for the patients.
(Innovations # 30-33: Surgery for small and large intestines)
Cancer and Feeding Associated surgery
“Reaching out to our fellow human beings in their time of real need with love and humility is paramount” – Professor Amir Nisar
30
LAFJ (Laparoscopic Assisted Feeding Jejunostomy) under local anaesthetic.
Laparoscopic is performed under local anaesthetic only and feeding jejunostomy tube is placed. This is very helpful for patients who are unfit for general anaesthetic, obstructed pharynx and those who can not have an endoscopy as well.
Lesions in Duodenum and proximal jejunum are generally inaccessible for diagnosis and treatment. The complexity is compounded if there is an element of obstruction as well. This innovative technique simplifies the management of lesions in the “Dragon’s Territory”(Term phrased by Professor Amir Nisar for Duodenum and DJ flexure.)
Innovation dealing with complex Small intestine pathologies:
“When all physicians from all specialties fail in a hospital to deal with these complex situations, then these two innovations walk the walk” – Professor Amir Nisar
32
LAE (Laparoscopic Assisted Enteroscopy) for complex and troublesome small bowel lesions, tumors, telangiectasias and strictures.
(Innovations # 34-38: Surgery of Oesophagus and Stomach)
34
Esophageal and Stomach cancer surgery
“Once in a lifetime Eureka moment for this amazing innovation; Thanks to Allah”
“Holy Plane” in chest for Laparoscopic and open esophageal and esophagogastric cancer resection surgery; improving resection margins and potentially reducing local recurrence.
35
Laparoscopic Merendino’s Surgery
“ The Gold Standard to treat reflux after Weight Loss Surgery ”
Two approached for this complex surgery for GIST lesions or early cancer and other conditions of the Gastro Oesophageal Junction.
“A condition presenting itself in one of the most inaccessible and complex areas in the body: simplified with these innovations; Life Saving innovations indeed!” – Professor Amir Nisar
36
Laparoscopic / Intragastric Hybrid management of Gastric Bleeding Dieulafoy Lesion
An Innovation for dealing with life threatening Gastric Bleeds from GISTS or Dieulafoy
“Series of steps, operative techniques/variations and strategies to ensure standardized surgery to the highest level, minimizing risks & complications: reducing operative time and improving outcomes”
Anti-Reflux Surgery
Series of crucial steps and minor innovations to make the surgery safe and reduce the risk of complications; namely dysphagia, recurrent reflux, wrap migration and wrap slippage
Anti-Reflux Surgery after Weight Loss Surgery
Multiple steps to ensure good outcomes and to avoid reflux after surgery
Inguinal hernia surgery
Some refined steps and innovative techniques to deal with complex and simple scenarios to ensure excellent long-term outcomes with swift post operative reviver
Gall Bladder Surgery
Key steps in surgery to ensure safe surgery and avoiding major complications like common bile duct injury, hepatic artery injury and conversions to open operations.
Appendicectomy surgery Protocol
Crucial considerations and steps to avoid complications like Bleeding, bowel damage, post operative infections and abscesses after this common surgery.