
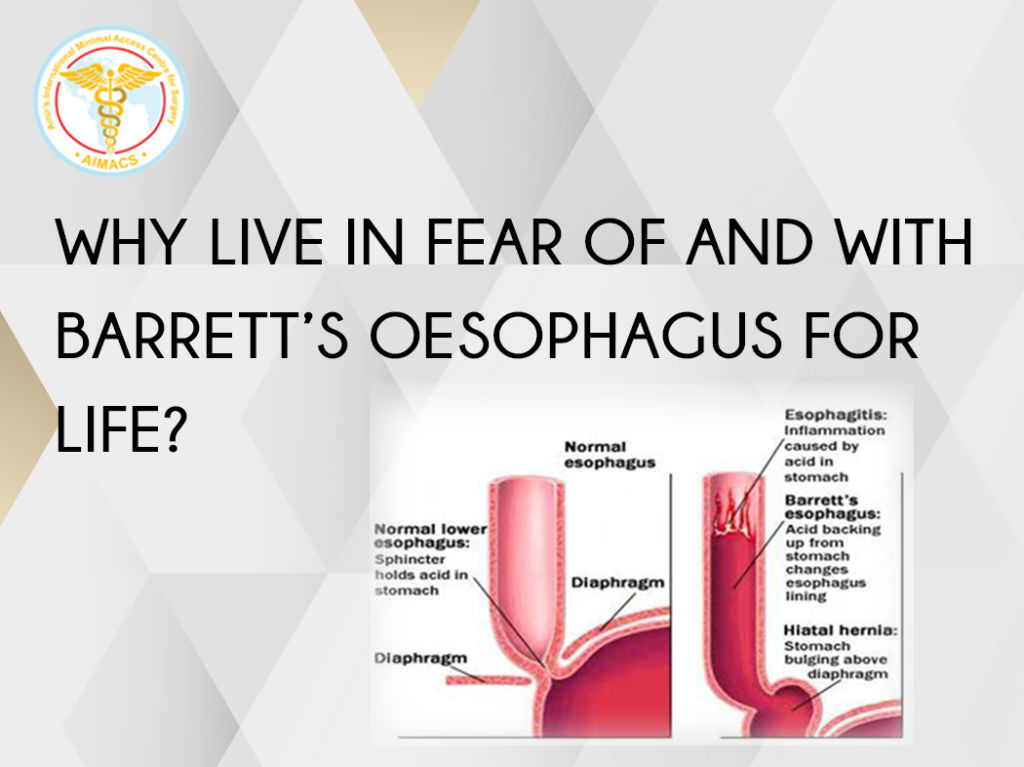
Why live in fear of and with Barrett’s Oesophagus for life?
Prevention is better than cure.
“Amir’s Barrett’s Protocol”
Author has 30 years’ experience of Laparoscopic surgery. He is a teacher and trainer in United Kingdom, Europe, Middle East and Asia in Gall Bladder disease surgery
A famous retired footballer from New Castle upon Tyne, United Kingdom expressed his gratitude in his flowery interview in Newspaper for his surgeon. The surgeon diagnosed him with Barrett’s Oesophagus (Change in the lining of the Oesophagus which can further change into cancer of food pipe).

After years of surveillance it did change into cancer.
The surgeon proceeded with major surgery (Open Ivor Lewis Oesophagectomy), cutting open the abdomen and chest of the patient and successfully removed the cancer.
Patient lived on, with cancer cured to tell his tale and express his gratitude to the surgeon who saved his life!
QUESTION : Did the surgeon actually do any favour to his patient?

About one third of general population suffers from Reflux of acid or acid and bile refluxing upwards from the stomach into the food pipe. About 15% of the population have its more severe form by giving them heartburn or volume reflux (acid/bile/food in mouth) on regular basis. These patients require to take regular medicines to suppress acid production in stomach. There is no suppression medicine for the bile!
In some cases, these medicines help, in others the disease may keep progressing despite taking medication.
Acid is injurious to Oesophagus lining but in the absence of acid, bile that cannot be neutralized and altered, becomes even more injurious to the oesophagus and can cause cancer itself. A fact ignored or missed by many family consultants, gastroenterologists and surgeons alike.
The treatment with medication is helpful and required in all these patients and remains the mainstay of Reflux management and Barrett’s changes in Oesophagus. However, the treating doctors must have his fingers on the pulse all the time; lest in case of ineffective medical treatment the disease may keep progressing under their vigilant care.
Once it becomes cancer then the only treatment is in the form of surgery where a major operation is carried out by opening the abdomen and the chest; and/or neck of the patient.
Cancer is removed but patient’s quality of life is much poorer than before. Patients accept it as they are grateful for having their life saved, like the famous footballer.
One of the aftermaths of surgery is persistent, severe and debilitating reflux; the start of the whole issue in the first place.
Before surgery the patient went through Heartburn ⇒ Reflux ⇒ Cancer.

The new ‘ VICIOUS ’ cycle after surgery is :
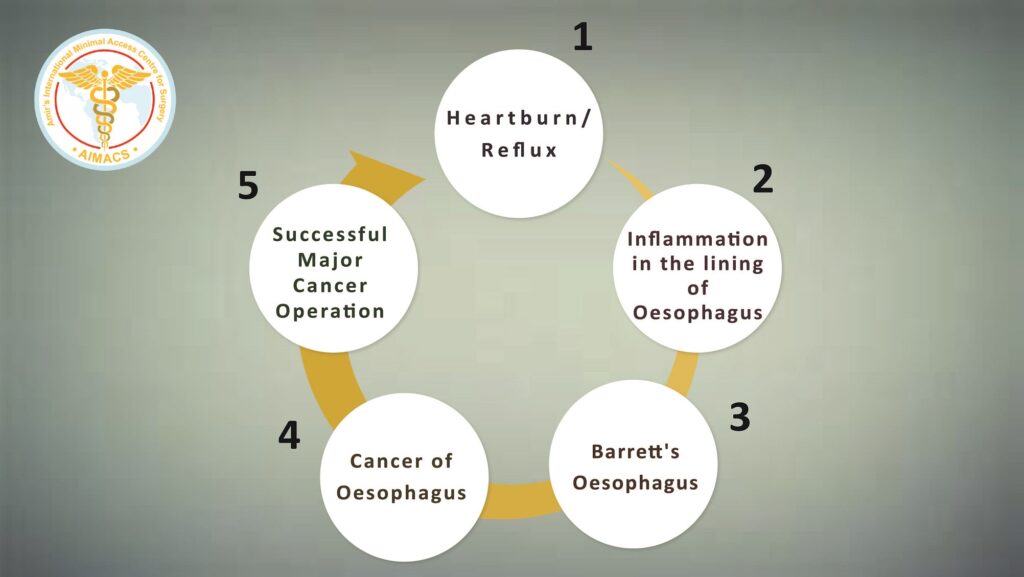
Where did the physician go wrong or missed the opportunity in this cycle?
The answer is simple: at stage 2 and 3.
A typical story of missed opportunities, repeated time and time again, all over the world and especially in our so-called developed countries at the pinnacle of their medical care, expertise and facilities.
Algorithms, which are practical and logical to follow are:
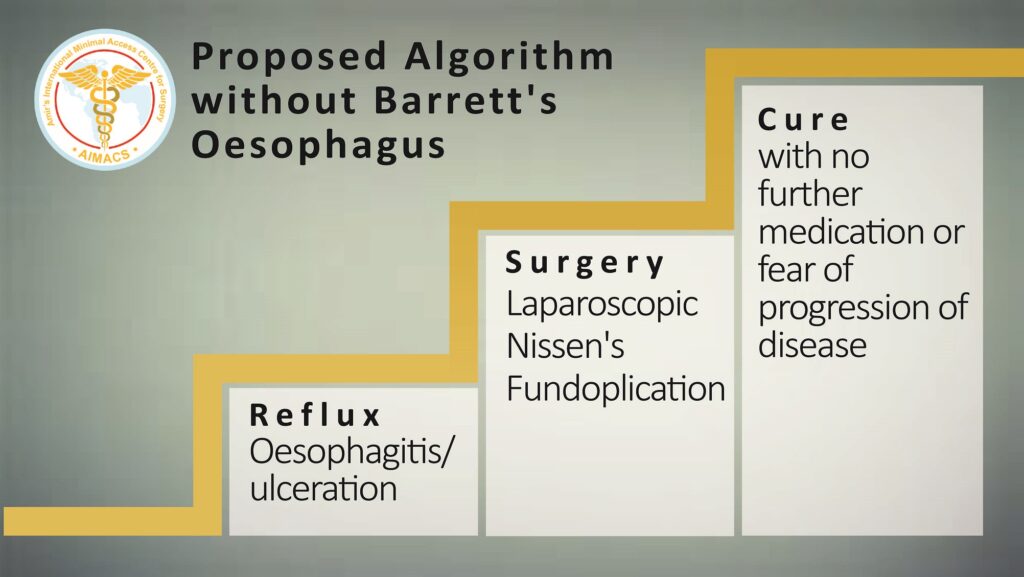
First alogrithym (for Reflux and Oesophagitis without Barrett’s Oesophagus) provides a logical approach to identify and treat the root cause of cancer of oesophagus.
- Patient once diagnosed with GORD/GERD is prescribed medication for short term (3-6 months and improvement is monitored.
- Oesophageal Physiological studies are performed by the gastroenterologist to quantify reflux and assess the motility of oesophagus.
- Surgeon assesses the patient for his suitability for Laparoscopic Nissen’s Fundoplication.
- Surgery is carried out general anaesthetic as one-night stay in the hospital. All medication is stopped and patient is discharged from any further follow up.
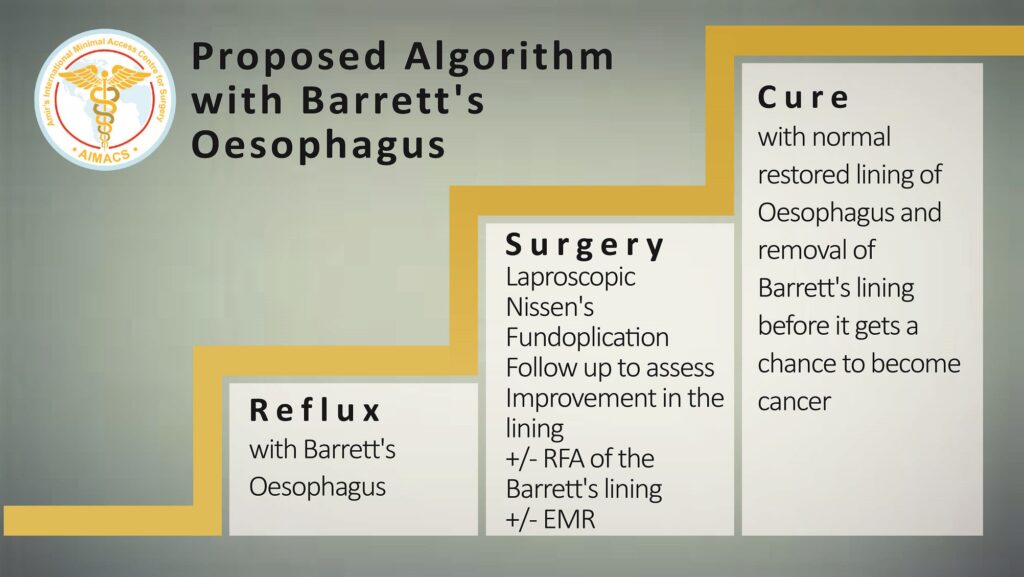
The rationale of this second algorithm for patient diagnosed with Barrett’s Oesophagus:
- When a patient is diagnosed with Barrett’s Oesophagus. He should have an endoscopy by the gastroenterologist and biopsies of the area for confirmation.
- Once diagnosis is confirmed, then he should have his oesophageal physiological studies and following that, see a surgeon to discuss the option of Laparoscopic Nissen’s Fundoplication.
- A repeat gastroscopy/endoscopy should be done 1 year after the surgery to assess the stability or improvement in the Barrett’s lining:
a) In some cases, the normal lining of the oesophagus will be restored.
b) If there is no change back to normal lining, then the options are:
(i) Radio Frequency Ablation (RFA) treatment in the form of Halo should be carried out. This ablates the Barrett’s lining and new lining regenerated will be normal lining of oesophagus
(ii) EMR (Endoscopic Mucosal Resection), is another option in appropriate cases
4. Patient should remain under the gastroenterologist’s surveillance gastroscopy programme once every three years.
5. After two to three consecutive normal endoscopies and biopsies, if the gastroenterologist is satisfied with the stable condition of the patient then the patient could be discharged from any further gastroscopy or biopsies. Another option is to offer a repeat gastroscopy after five years.
6. The great benefit of this structured approach for the patients is threefold:
a) Not living on medication for life with fear of developing a cancer
b) Enjoying a better quality of life after surgery with no reflux and no side effects of the medicines
c) Arresting the disease process and getting a cure rather than knowingly going down a slippery and at times life threatening slope.
Disclaimer: Barrett’s Oesophagus, Oesophagitis, Reflux disease, GORD/GERD, Laparoscopic Nissen’s Fundoplication surgery are all very complex scenarios. Patients and doctors must consider taking advice from expert surgeons and gastroenterologists in this field for the whole range of management options and take responsibility for their own decisions.
This article may provide some food for thought to the clinicians and general public; however, following any suggestion mentioned in the article here should be very carefully evaluated by the experts or general public. Every case needs to be assessed on its own merit.